Why Some Fat Deposits Are Resistant to Diet and Exercise: The Biology of Stubborn Fat
Discover why certain areas of your body stubbornly resist diet and exercise. Learn the biological reasons behind resistant fat deposits in the abdomen, hips, thighs, and flanks, and how non-invasive fat reduction can help.
You've been eating well, exercising regularly, and maintaining a caloric deficit, yet certain areas of your body stubbornly refuse to lose fat. Your abdomen, hips, thighs, and flanks seem to hold onto fat deposits despite your best efforts. This frustrating reality isn't a personal failure or lack of willpower. It's biology.
Stubborn fat deposits exist because different areas of your body store fat differently. Hormones, genetics, fat cell distribution, and circulation patterns create biological "fat storage zones" that are metabolically resistant to diet and exercise alone. Understanding the science behind stubborn fat helps explain why these areas persist and introduces modern solutions like non-invasive fat reduction technologies.
The Biology of Stubborn Fat: Why Certain Areas Resist Weight Loss
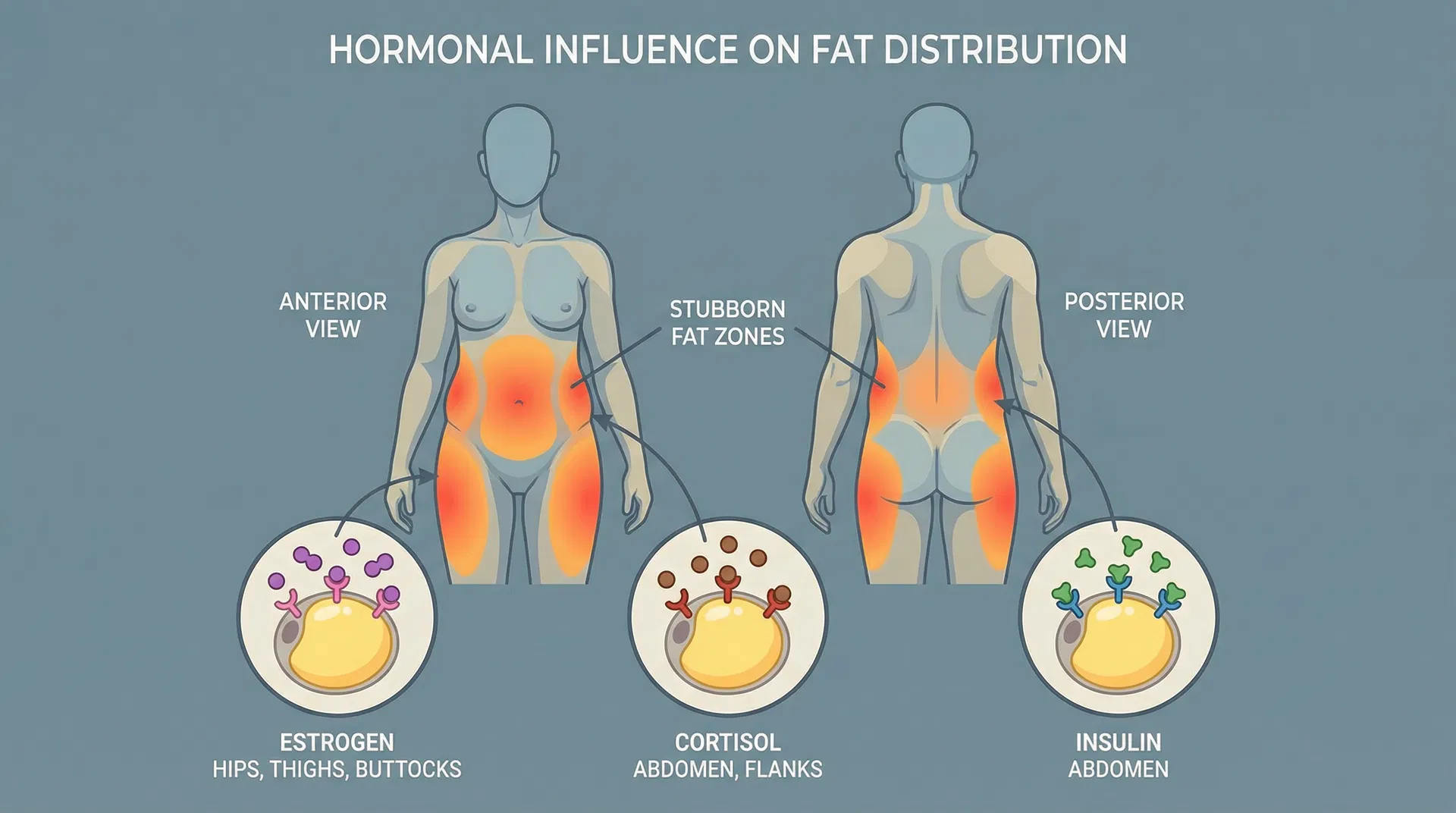
Hormonal Influence on Fat Distribution
Hormones are master regulators of where your body stores fat. Three hormones in particular determine which areas become stubborn fat zones: estrogen, cortisol, and insulin.
Estrogen preferentially directs fat storage to the hips, thighs, and buttocks, particularly in women. This is why women often notice stubborn fat in these lower body areas even when their overall body fat percentage is low. This hormonal pattern developed evolutionarily to support reproductive health and energy reserves for pregnancy and lactation.
Cortisol, the stress hormone, drives fat accumulation in the abdominal region and flanks. During chronic stress, elevated cortisol levels signal your body to store energy as visceral fat (deep abdominal fat) and subcutaneous abdominal fat. This is why stress management is crucial for reducing stubborn belly fat, and why people under chronic stress often develop abdominal weight gain despite maintaining their usual diet and exercise routine.
Insulin sensitivity also varies by body region. The abdomen and flanks are particularly insulin-sensitive, meaning fat cells in these areas readily absorb and store triglycerides when insulin levels are elevated. This explains why refined carbohydrates and high-sugar foods disproportionately contribute to stubborn abdominal fat accumulation.
Genetic Predisposition and Fat Cell Distribution
Your genetics largely determine your personal fat distribution pattern. Some people are genetically programmed to store more fat in their lower body, while others accumulate it primarily in the abdomen. This genetic blueprint is established early in life and remains relatively stable throughout adulthood.
Additionally, stubborn fat areas often contain a higher density of fat cells. The abdomen, hips, thighs, and flanks typically have more adipocytes (fat cells) than other body regions. More fat cells means more storage capacity and more biological machinery dedicated to storing fat rather than releasing it.
Genetics also influence the types of fat cells present in different regions. Some areas contain predominantly white adipose tissue (storage fat), while other regions have more brown adipose tissue (metabolically active fat that burns calories for heat). Stubborn fat zones tend to have higher concentrations of white adipose tissue, making them metabolically resistant.
Metabolic Differences Between Fat Cell Types
Not all fat cells are created equal. The body contains two primary types of adipose tissue with dramatically different metabolic properties: visceral fat and subcutaneous fat.
Visceral fat (intra-abdominal fat) is metabolically active and contains high mitochondrial density, robust blood vessel networks, and abundant sympathetic nerve innervation. Despite being metabolically active, visceral fat is also metabolically flexible and responsive to diet and exercise changes. However, the abdomen also contains significant subcutaneous fat deposits that behave differently.
Subcutaneous fat (fat stored directly under the skin) in stubborn areas like the lower abdomen, flanks, hips, and thighs has lower mitochondrial density, fewer blood vessels, and reduced sympathetic nerve innervation. This metabolic profile makes these fat cells resistant to mobilization and breakdown, even during caloric deficit and exercise.
The key difference lies in metabolic enzyme activity. Stubborn fat cells have reduced hormone-sensitive lipase (HSL) activity, the primary enzyme responsible for breaking down stored triglycerides into free fatty acids that can be burned for fuel. Simultaneously, these cells often have elevated lipoprotein lipase (LPL) activity, an enzyme that promotes fat uptake and storage. This enzymatic imbalance creates a metabolic environment that favors fat storage over fat mobilization.
Circulation and Blood Flow Differences
Stubborn fat areas have consistently lower blood flow compared to other body regions. The abdomen, flanks, hips, and thighs receive fewer blood vessels per unit of adipose tissue, limiting oxygen delivery and nutrient transport to fat cells in these areas.
This circulatory limitation has profound metabolic consequences. Fat mobilization requires adequate blood flow to deliver hormonal signals (like norepinephrine) that trigger lipolysis. Reduced blood flow means these mobilization signals reach stubborn fat cells less effectively. Additionally, poor circulation limits the removal of released fatty acids from the tissue, reducing the efficiency of fat breakdown.
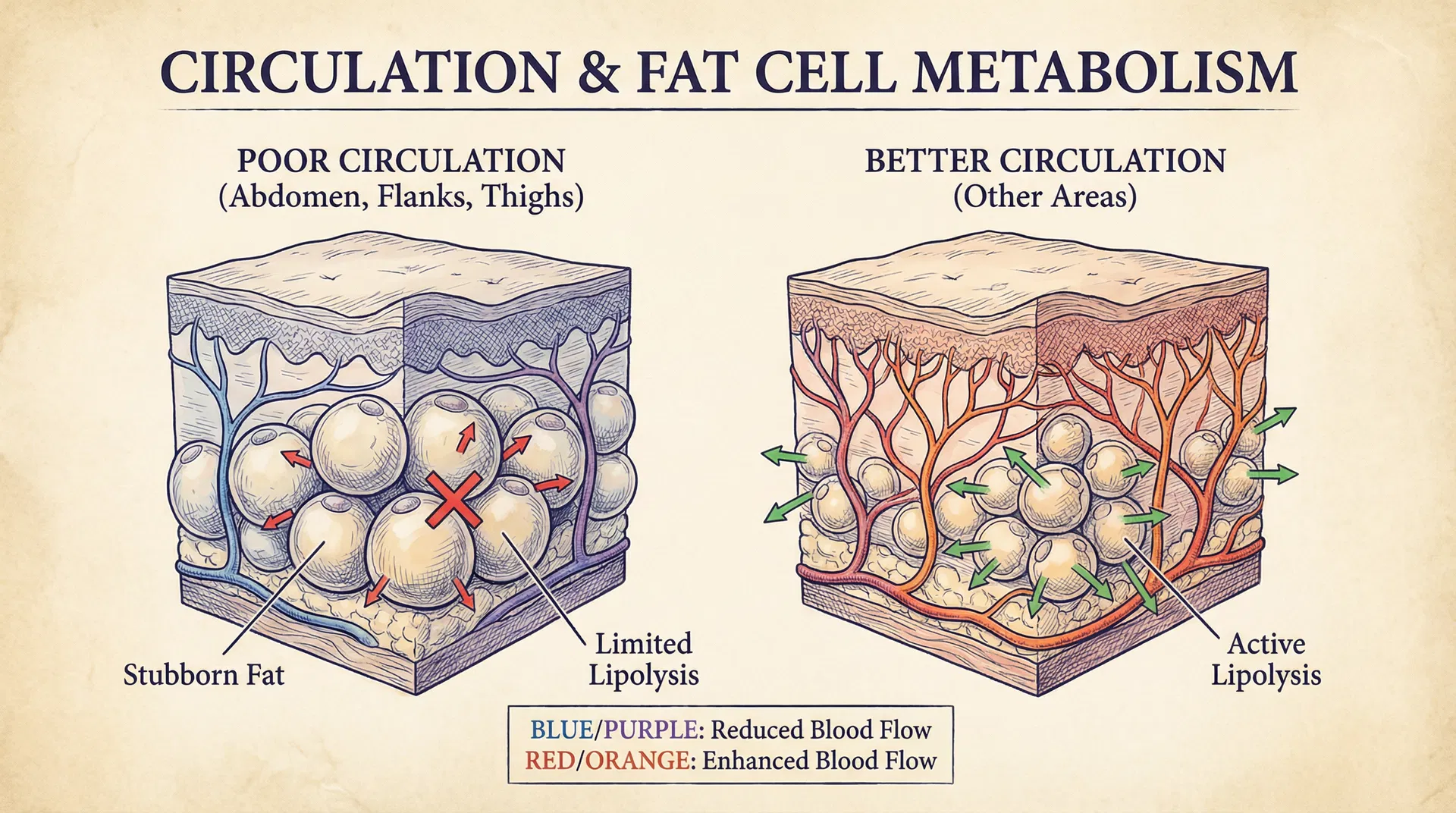
The sympathetic nervous system, which controls fat mobilization through beta-adrenergic receptors, also shows reduced innervation in stubborn fat areas. This means fat cells in these regions receive fewer "break down fat" signals compared to more metabolically responsive areas.
Adrenergic Receptor Imbalance
Fat cells contain two types of adrenergic receptors that have opposing effects on lipolysis: beta-3 adrenergic receptors (which promote fat breakdown) and alpha-2 adrenergic receptors (which inhibit fat breakdown).
Stubborn fat cells have a problematic receptor imbalance. They contain fewer beta-3 receptors (the "fat-burning" receptors) and more alpha-2 receptors (the "fat-storage" receptors). This receptor distribution means that even when norepinephrine levels are elevated during exercise or stress, the signal to break down fat is muted in stubborn areas while the signal to store fat remains strong.
This receptor imbalance is particularly pronounced in women's lower body fat deposits and in abdominal fat cells of both sexes. It's a primary reason why targeted fat loss through diet and exercise alone is nearly impossible in these regions.
Modern Solutions for Stubborn Fat: Non-Invasive Fat Reduction Technologies
Understanding the biology of stubborn fat reveals why diet and exercise alone are insufficient for reducing these deposits. Modern non-invasive fat reduction technologies work by targeting the specific biological mechanisms that make fat resistant to mobilization.
How Non-Invasive Fat Reduction Works
Non-invasive fat reduction technologies employ several mechanisms to reduce stubborn fat:
Cryolipolysis (cold laser fat reduction like Zerona) works by selectively cooling adipose tissue to temperatures that trigger apoptosis (programmed cell death) in fat cells. Because fat cells have a lower freezing point than surrounding tissues, they can be destroyed without damaging skin, nerves, or muscle. The body then naturally eliminates the dead fat cells through lymphatic drainage over several weeks.
Radiofrequency and ultrasound technologies generate heat within adipose tissue, increasing fat cell temperature to levels that cause cell death. These modalities also stimulate collagen remodeling and improve skin texture while reducing fat deposits.
Laser-assisted fat reduction uses specific wavelengths of light to penetrate skin and adipose tissue, disrupting fat cell membranes and triggering lipolysis. Some laser systems also stimulate lymphatic drainage, enhancing the removal of released fatty acids and dead fat cells.
The advantage of these technologies is that they bypass the biological resistance mechanisms that make diet and exercise ineffective for stubborn fat. Rather than attempting to mobilize fat through hormonal signals and exercise, these devices directly damage fat cells, forcing their elimination regardless of adrenergic receptor imbalance, poor circulation, or unfavorable metabolic enzyme ratios.
Why Non-Invasive Fat Reduction Succeeds Where Diet and Exercise Fail
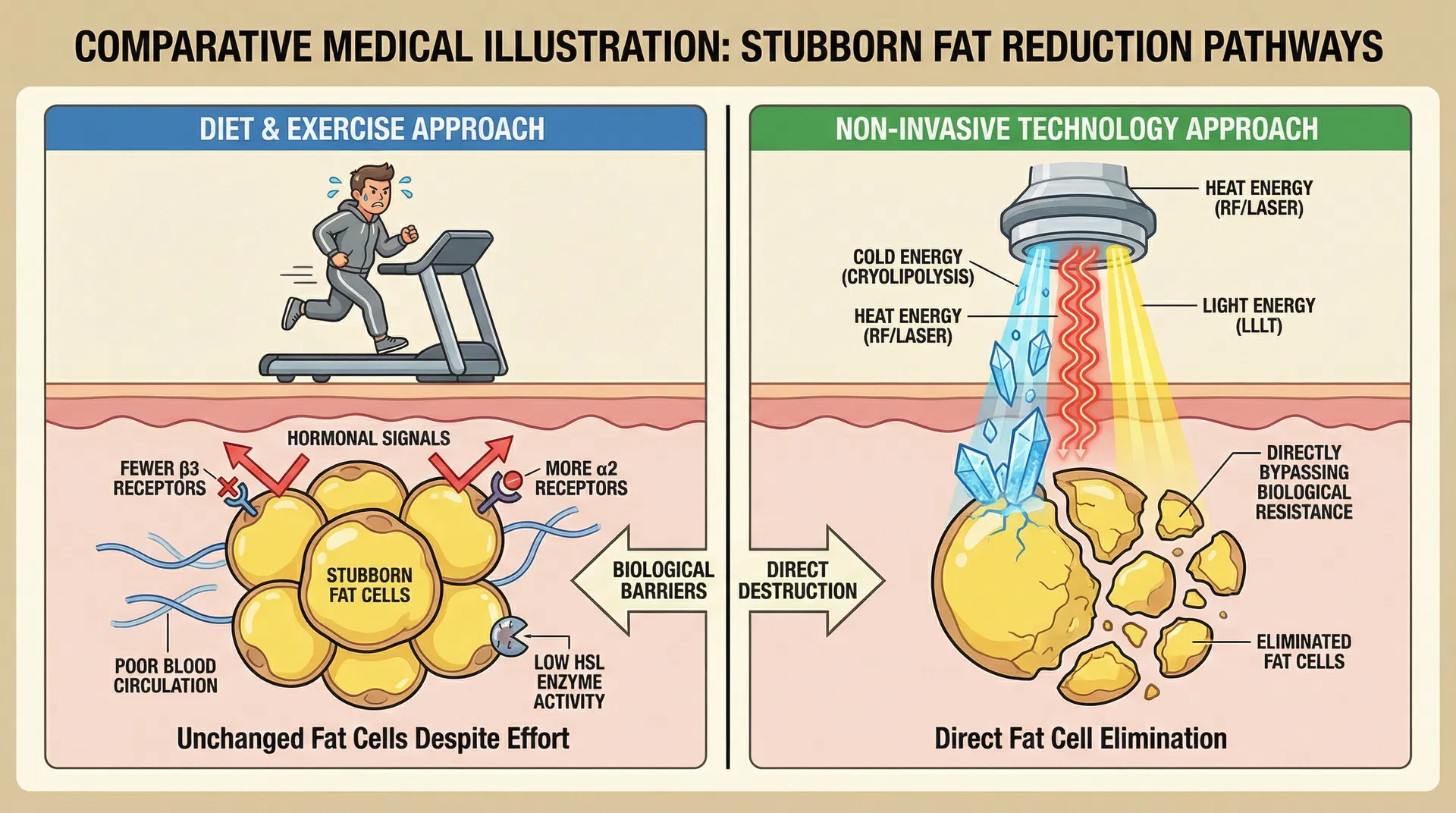
Stubborn fat deposits resist diet and exercise because of reduced beta-3 adrenergic receptors, elevated alpha-2 adrenergic receptors, low hormone-sensitive lipase activity, high lipoprotein lipase activity, poor blood circulation, and low mitochondrial density.
Non-invasive fat reduction technologies eliminate these barriers by directly destroying fat cells through cold, heat, or light energy. The technology doesn't rely on hormonal signaling, exercise-induced mobilization, or metabolic enzyme activity. Instead, it simply damages fat cell membranes beyond repair, triggering cell death and removal.
This is why patients often see results with non-invasive fat reduction in areas where diet and exercise have failed for years. The technology addresses the fundamental biological resistance of these fat deposits.
Combining Approaches for Optimal Results
While non-invasive fat reduction is highly effective for stubborn fat, combining it with lifestyle modifications enhances results. A healthy diet, regular exercise, stress management, and adequate sleep all support the body's natural fat elimination processes and prevent new fat accumulation in treated areas.
Additionally, maintaining a healthy overall body weight prevents the remaining fat cells from expanding to compensate for eliminated cells. After non-invasive fat reduction treatment, the number of fat cells in treated areas is permanently reduced, but remaining cells can still enlarge if caloric intake exceeds expenditure.
Conclusion
Stubborn fat deposits are not a personal failure or sign of insufficient effort. They're the result of specific biological mechanisms: hormonal preferences for certain body regions, genetic predisposition, unfavorable fat cell metabolic profiles, poor blood circulation, and adrenergic receptor imbalances.
These biological factors make diet and exercise alone insufficient for reducing stubborn fat in areas like the abdomen, flanks, hips, and thighs. Modern non-invasive fat reduction technologies bypass these biological barriers by directly eliminating fat cells, providing results where traditional weight loss methods have failed.
For residents of Scottsdale seeking to reduce stubborn fat deposits, non-invasive fat reduction offers a science-based solution that addresses the underlying biology of resistant fat. Combined with healthy lifestyle choices, these treatments can help achieve the body contouring results that diet and exercise alone cannot provide.
Ready to explore this treatment?
Schedule Your ConsultationFrequently Asked Questions
Why can't I lose fat in my lower abdomen despite exercising regularly?
Lower abdominal fat is highly cortisol-responsive and insulin-sensitive, with reduced blood flow and unfavorable adrenergic receptor ratios. These biological factors make this area resistant to mobilization through diet and exercise alone. Non-invasive fat reduction directly targets these resistant fat cells.
Is stubborn fat the same as visceral fat?
No. Visceral fat (deep abdominal fat) is metabolically active and relatively responsive to diet and exercise. Stubborn fat typically refers to subcutaneous fat deposits with poor blood flow and unfavorable metabolic profiles. Both can be problematic, but they respond differently to interventions.
Can genetics determine where I store stubborn fat?
Yes. Genetics largely determine your personal fat distribution pattern and the metabolic characteristics of fat cells in different regions. If your parents stored fat in their abdomen or lower body, you're likely to have a similar pattern.
How long does it take to see results from non-invasive fat reduction?
Results typically appear gradually over 2-3 months as the body eliminates dead fat cells through lymphatic drainage. Some patients see initial changes within 2-3 weeks, with continued improvement over subsequent months.
Will treated fat return after non-invasive fat reduction?
The fat cells destroyed by non-invasive fat reduction are permanently eliminated. However, remaining fat cells can enlarge if caloric intake exceeds expenditure. Maintaining a healthy diet and exercise routine prevents new fat accumulation.
Can I target fat loss to specific body areas with diet and exercise?
Targeted fat loss is not possible through diet and exercise alone. Your body determines where fat is mobilized based on hormonal and genetic factors. Non-invasive fat reduction is the only proven method for targeted fat elimination.
Why do women tend to store more stubborn fat in the hips and thighs?
Estrogen preferentially directs fat storage to the hips, thighs, and buttocks. These areas develop high fat cell density during puberty and remain metabolically resistant due to unfavorable adrenergic receptor ratios and poor blood circulation.
Is non-invasive fat reduction safe for all body areas?
Non-invasive fat reduction is safe for most body areas where fat deposits are present. However, treatment should be performed by qualified professionals who understand the anatomy and can safely deliver the appropriate energy levels to adipose tissue without damaging surrounding structures.

